Neck strains and sprains are some of the most common musculoskeletal injuries. Neck pain from acceleration and deceleration injuries after a car crash is often called Whiplash Syndrome or Whiplash Associated Disorder (WAD).
Neck Anatomy
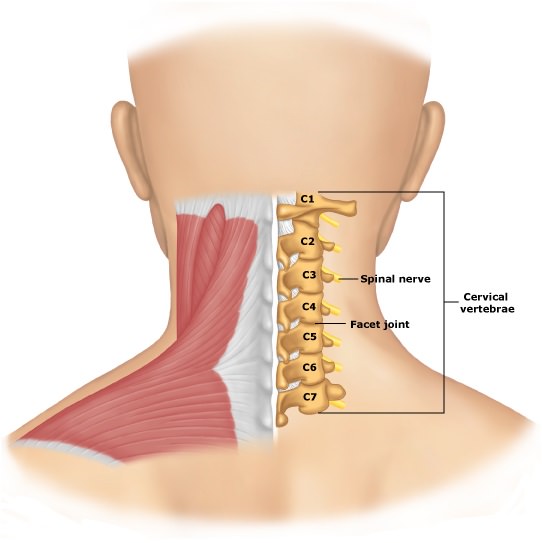
The neck consists of seven cervical vertebrae stacked on top of each other and separated by intervertebral discs. The top two vertebrae are specialised for head rotation and flexion/extension (bending forwards and backwards).
The head is heavy and is balanced on top of the slender column of the neck vertebrae. This makes it vulnerable to sudden forces as the head magnifies the effects of stresses on the neck.
Who Gets A Cervical Strain Or Whiplash?
Chronic stresses and strains on the neck are thought to account for around 85% of neck pain problems. These may be related to repetitive lifting, pulling something heavy, awkward sleep posture or sitting in a poor position for long periods looking at a computer screen.
Whiplash injuries from rear-end car collisions are common at about one case per 1000 people per year. Whiplash syndrome is responsible for significant on-going neck pain and disability and for large costs to society.
Cervical Sprain And Whiplash Symptoms
- Neck pain may occur at the time of the accident or come on in the succeeding 12 to 72 hours
- Headache, especially at the back of the head, termed occipital headache
- Muscle spasm as the muscles try and hold the painful parts still
- Neck, upper back, shoulder and arm pain may be present
- Dizziness and tinnitus may occur
- Weakness of the arms, sleep problems and altered memory and concentration may also occur.
Cervical Sprain and Whiplash Treatment
Early rehabilitation is important to reduce the chances of long-term disability and chronic pain. A physiotherapist may use passive treatments, to begin with, although research has shown that active treatment should be progressed to as soon as possible.
Typical passive physiotherapy treatments include ice, heat, massage, neck traction, joint mobilisations and traction. Passive treatments should prepare the patient for the active treatments such as neck exercises, stretches and fitness work.
The focus of physio is to increase function of the neck and upper body and reduce the chances of a chronic problem, encouraging the patient to return to work as soon as they can. Complete pain relief before going back to work is not appropriate as early return to work is associated with improved outcome.
Strengthening of the deep postural muscles of the neck has been shown to improve functional ability and active physiotherapy has been shown to be more cost effective than other approaches.
Manipulation and other forms of manual therapy have been shown to have some usefulness in more chronic whiplash and cervical sprain conditions.
Surgery is not indicated for whiplash or cervical sprain unless there is spinal cord or nerve root compression.
In persistent cases, radiofrequency neurotomy may be used. This technique is used when pain has been shown to come from one or more facet joints. By blocking the nerves from those joints the nerve transmission is altered. The neurotomy damages the nerves and reduces or abolishes their ability to transmit pain.
Other treatments include pain management programmes, botulinum injections, steroid injections and traction.
References:
- Neck pain and stiff neck. NHS Choices. http://www.nhs.uk/conditions/Neck-pain/Pages/Introduction.aspx
- Neck pain – whiplash injury. NICE. http://cks.nice.org.uk/neck-pain-whiplash-injury#!topicsummary
Last Review Date: 11-12-2019
Next Review Date: 09-12-2021
{kind=link}